Antimicrobial Resistance: Ara Darzi’s Case for Urgent Action
Antimicrobial resistance is no longer a niche public health issue. It is a mounting systems problem that affects hospitals, routine surgery, cancer care, and infection control across the board. In the WIRED Health 2026 discussion, Ara Darzi makes the case that antimicrobial resistance needs far more political focus and operational follow-through. That matters to you because once antibiotics stop working, modern medicine gets riskier fast. A simple infection can turn serious. A standard procedure can carry a higher chance of harm. And health systems that already run hot face another layer of pressure. The real question is not whether antimicrobial resistance is serious. It is whether leaders will treat it with the urgency they usually reserve for a visible crisis.
What matters most
- Antimicrobial resistance threatens basic medical care, not only rare or complex cases.
- Darzi’s message points to a policy gap as much as a medical one.
- Hospitals need better stewardship, cleaner data, and tighter infection prevention.
- Drug development matters, but smarter use of existing antibiotics matters just as much.
Why antimicrobial resistance is a health system problem
People often hear “drug-resistant infection” and picture a difficult case in an ICU. That is too narrow. Antimicrobial resistance changes the risk profile of huge parts of medicine, including childbirth, joint replacements, organ transplants, and chemotherapy support.
If antibiotics fail more often, doctors lose one of their basic safety nets. Think of it like a building with weakening fire doors. The structure still stands for a while, but every corridor becomes less safe.
Modern medicine depends on antibiotics working when needed. Once that assumption breaks, routine care stops being routine.
That is why Darzi’s warning lands. He is not talking about a distant laboratory issue. He is pointing at a service-wide threat with economic and human costs attached.
What Ara Darzi is really pushing leaders to do
Darzi has long focused on how health systems perform under strain, and this debate fits that pattern. His argument is not simply “fund more science.” It is “treat antimicrobial resistance like a cross-system failure risk.” That is a sharper and more useful frame.
Look, policy conversations often split this issue into neat boxes. Research sits in one box. Hospital prescribing sits in another. Global health sits somewhere else. Real life does not work that way.
Leaders need to connect four threads at once:
- Reduce unnecessary antibiotic use in humans.
- Track resistance patterns with better surveillance.
- Improve infection prevention in hospitals and communities.
- Create incentives for new antibiotics and diagnostics.
Miss one, and the whole effort gets weaker. That is the frustrating part.
Why antibiotic stewardship still gets underplayed
Antibiotic stewardship sounds technical, even bureaucratic, so it rarely grabs headlines. But it is one of the few tools health systems can act on now. And yes, now matters more than slogans about future breakthroughs.
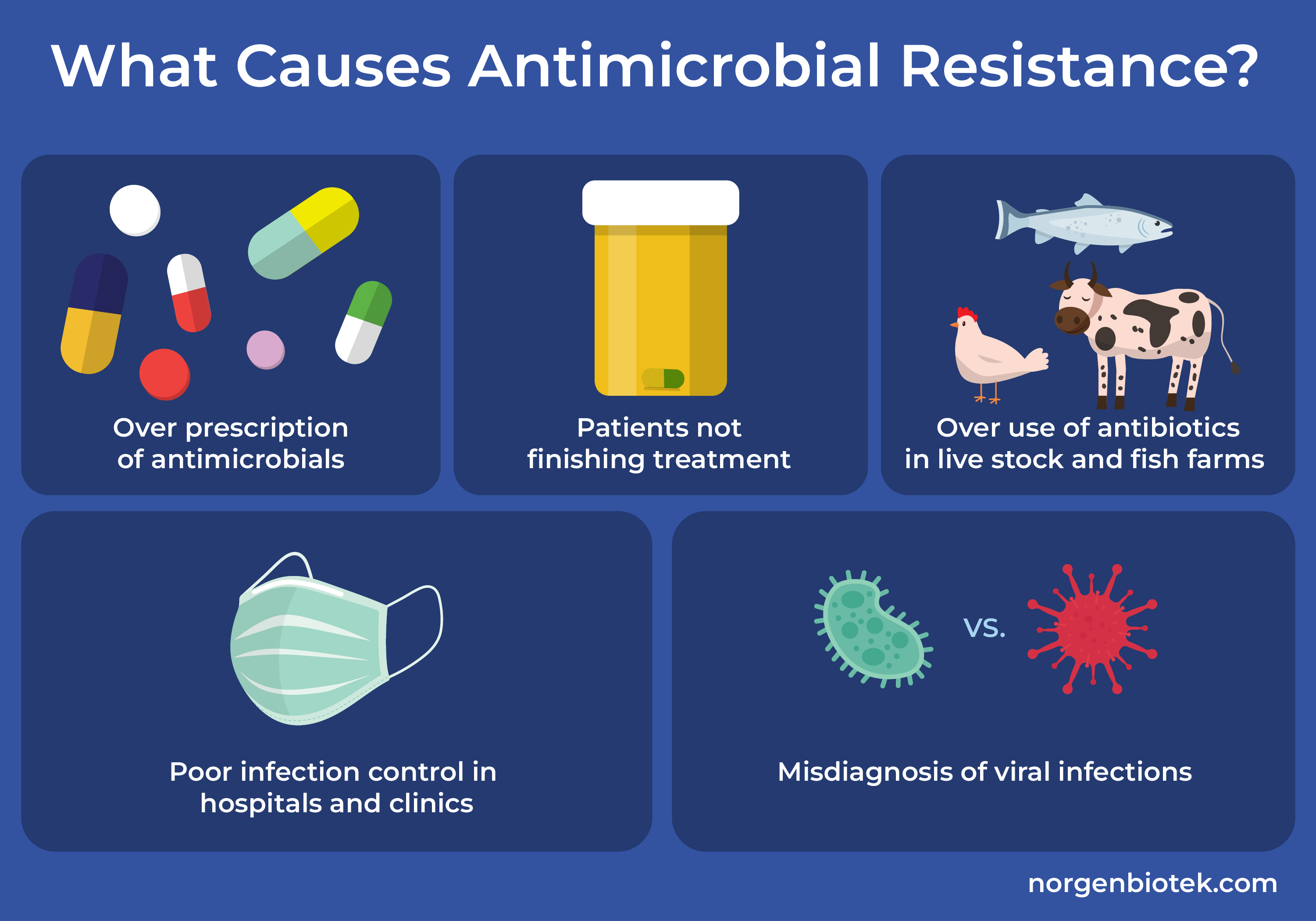
Good stewardship means the right drug, at the right dose, for the right duration. It also means not prescribing antibiotics when they will not help, such as many viral infections. Easy to say. Harder to enforce in overloaded clinics, where time is short and patient expectations can push prescribing in the wrong direction.
One sentence matters here.
Overuse is the part of antimicrobial resistance we can control most directly.
According to the World Health Organization, antimicrobial resistance is among the top global public health threats, and misuse of antimicrobials is a major driver. That should settle the debate over whether stewardship is optional. It is not.
Antimicrobial resistance needs better data, not more guesswork
Here is a problem that gets less attention than it should. Many health systems still struggle to collect, share, and act on resistance data quickly enough. If clinicians do not know local resistance trends, prescribing becomes a patchwork of habit and probability.
That is dangerous.
Fast diagnostics can help by showing what pathogen is involved and whether an antibiotic is likely to work. Better surveillance can help public health teams spot patterns across hospitals and regions. And cleaner data can guide procurement, prescribing rules, and outbreak response.
Honestly, this is where the gap between political talk and hospital reality shows up. Everyone says data matters. Fewer people want to pay for the plumbing behind it.
What stronger surveillance looks like
- Shared lab reporting across hospitals and clinics
- Regular local antibiograms for frontline prescribers
- Quicker alert systems for resistant outbreaks
- Links between prescribing data and patient outcomes
Without that foundation, antimicrobial resistance policy turns vague fast.
Prevention beats rescue
People tend to focus on the dramatic end of the story, which is the patient with a resistant infection and few treatment options. But the less flashy work often saves more lives. Infection prevention, sanitation, vaccination, and hospital hygiene reduce the need for antibiotics in the first place.
Why wait until the fire spreads if you can remove the fuel? That is the logic.
This includes basics that sound almost old-fashioned, such as hand hygiene, isolation protocols, and cleaner hospital workflows. It also includes vaccination programs that reduce bacterial complications and lower overall antimicrobial use. Public health is often treated as background noise until it fails. Then everyone notices.
The drug pipeline problem is real, but it is not the whole story
New antibiotics are still needed. Some bacteria have outpaced the medicines available, and the market for antibiotic development has been a poor fit for traditional pharma incentives. Companies do not make blockbuster returns from drugs that clinicians are supposed to use sparingly. That mismatch has been obvious for years.
But a bigger pipeline alone will not bail us out. If new drugs enter the market and old prescribing habits stay in place, resistance will catch up again. Fast.
New antibiotics buy time. They do not fix the behavior and system failures that created the problem.
That is why Darzi’s broader framing makes sense. Antimicrobial resistance is part innovation issue, part governance issue, and part discipline issue inside health systems.
What health leaders should do next on antimicrobial resistance
If you run a hospital, advise policymakers, or work in health operations, the short list is fairly clear:
- Make antibiotic stewardship a board-level metric, not a side program.
- Fund lab capacity and rapid diagnostics.
- Publish local resistance trends in formats clinicians can actually use.
- Strengthen infection prevention teams and audit compliance.
- Back payment models that support antibiotic R&D without encouraging overuse.
And if you are watching this as a citizen or patient, ask a simple question whenever leaders talk about health resilience. Are they treating antimicrobial resistance as core infrastructure, or as a specialist issue they can park for later?
The next test for serious health policy
Darzi’s warning should unsettle policymakers, because antimicrobial resistance exposes a habit governments know too well. They respond hardest to emergencies they can see on tonight’s news, while slower threats pile up in the background. This one has been piling up for years.
But there is still room to act if health systems stop treating the issue as somebody else’s lane. Better stewardship, sharper surveillance, stronger prevention, and smarter incentives are not abstract fixes. They are practical moves. The real test is whether leaders will act before routine medicine becomes a gamble.