LDL Gene Therapy and Cholesterol Treatment
High LDL cholesterol is still one of the biggest drivers of heart disease, and for many people the usual drugs are not enough. That is why interest in LDL gene therapy is rising fast. The idea sounds simple. Change the biology once, then keep LDL low for years. But the real story is more complicated, and that matters if you are trying to separate serious medicine from headline fuel. Is this the future of cholesterol treatment, or just another early step that still has a long road ahead? The answer depends on safety, durability, and who gets treated first. For now, you need the facts, not the hype.
What cholesterol treatment with LDL gene therapy promises
- Lower LDL for the long term without daily pills.
- Better adherence if patients do not have to remember frequent dosing.
- Potential help for people with familial hypercholesterolemia, who often struggle to reach target levels.
- A different path from statins and PCSK9 drugs, which lower LDL through ongoing medication.
That promise is why researchers and drug makers keep pushing. Current therapies work, but they rely on repeat use. Gene therapy aims to change the equation at the source, more like fixing the wiring in a house than repainting the walls every year (and that is a very different kind of medical bet).
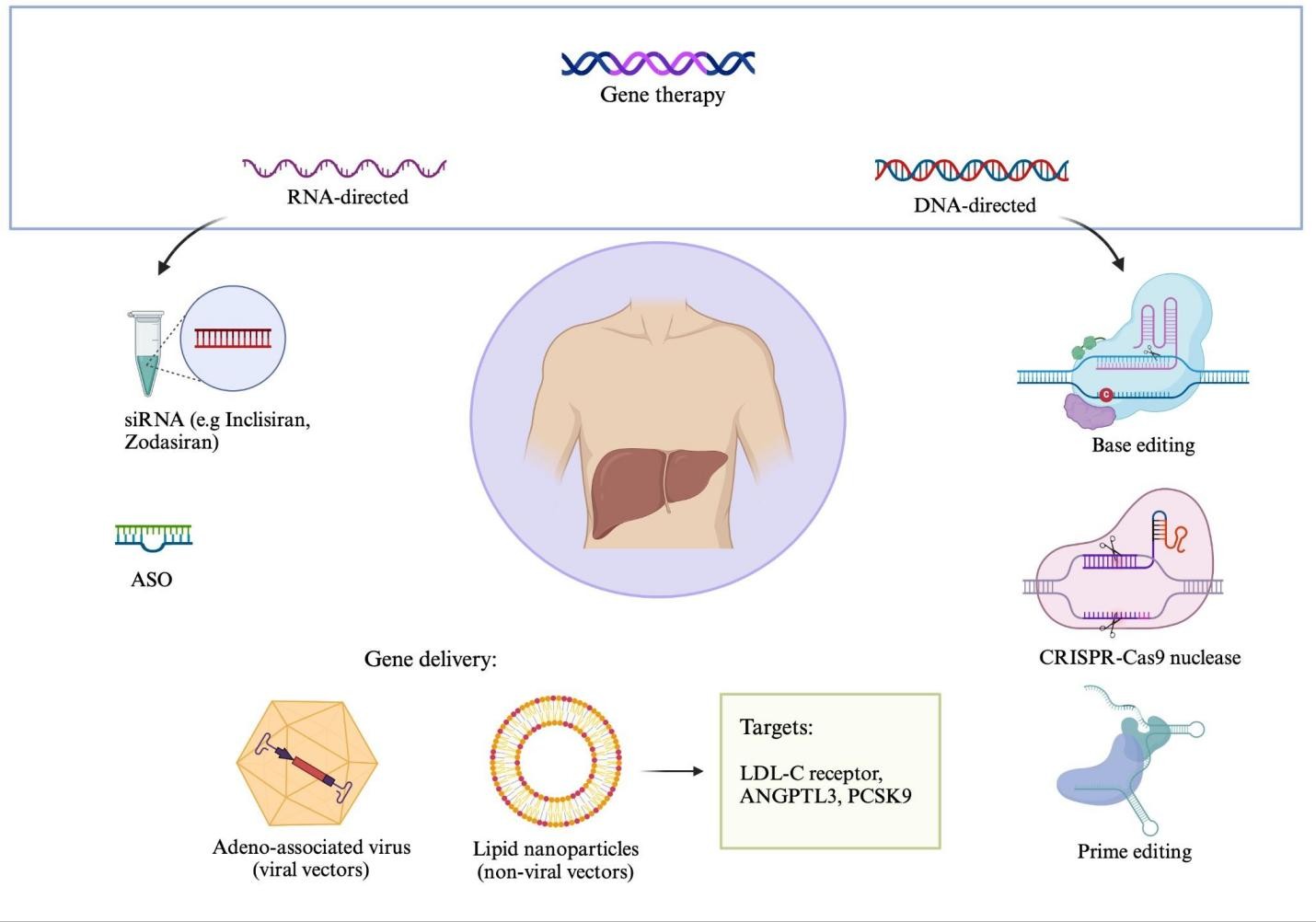
How LDL gene therapy is supposed to work
LDL gene therapy usually targets genes tied to cholesterol handling, such as PCSK9 or related pathways that affect how the liver clears LDL from the blood. The rough idea is to silence a harmful signal or add a helpful one so the liver removes more LDL over time.
That approach is appealing because the liver already does most of the heavy lifting. But biology is not a clean machine. Change one pathway and you can trigger side effects elsewhere. That is why early studies focus as much on safety as on LDL numbers.
“One treatment for lasting LDL control” sounds tidy. Human biology rarely is.
Why this matters for cholesterol treatment now
Heart disease remains the leading cause of death in the United States, according to the Centers for Disease Control and Prevention. LDL is one of the clearest risk factors doctors can modify. Lowering it helps, and the evidence for that is strong.
Statins remain the first-line treatment for most patients, with PCSK9 inhibitors, ezetimibe, and other drugs used when needed. But many people still do not hit their targets. Some cannot tolerate statins. Others stop taking medication. For them, a durable therapy could be a seismic shift.
Who might benefit first
- People with familial hypercholesterolemia.
- Patients who have very high LDL despite standard therapy.
- People with early cardiovascular disease and hard-to-control cholesterol.
- Patients who cannot stay on existing drugs because of side effects or adherence problems.
But broad use is a different question. A one-time therapy has to prove it can do more than lower a lab value. It has to prevent heart attacks, stroke, and death, and it has to do so without creating new problems.
What the science still has to prove
Researchers still need longer follow-up. Short-term LDL drops are useful, but they do not tell the whole story. Does the effect last for years? Does the body respond in ways that blunt the benefit? Are there delayed harms?
Those questions are non-negotiable. Gene therapy has a real history here. Some treatments have delivered major gains. Others have stumbled on delivery problems, immune reactions, or effects that fade faster than expected.
Cost will matter too. If the price is closer to rare-disease gene therapies than to common cardiovascular drugs, insurers may restrict access. That would limit use to the sickest patients first, which may be sensible medically, but frustrating for everyone else.
How LDL gene therapy compares with existing options
Think of cholesterol care like building a defensive line in football. Statins are the workhorse. PCSK9 inhibitors add another strong blocker. Gene therapy would try to change the team sheet itself. That sounds bold, but bold is not the same as proven.
- Statins lower LDL well and have decades of outcomes data.
- PCSK9 inhibitors are potent, but they require repeated dosing.
- Ezetimibe can help when statins are not enough.
- LDL gene therapy may offer longer control, but it still needs stronger evidence.
That is the comparison that matters. If a new therapy cannot beat or at least match the safety and outcomes of established drugs, it stays in the research lane. Fast LDL reductions alone do not close the case.
What you should watch next
If you follow cholesterol treatment, keep an eye on three things. First, the size and duration of LDL lowering in human trials. Second, whether researchers report serious side effects or immune issues. Third, whether trials show fewer cardiovascular events, not just prettier lab charts.
One more thing: pay attention to who gets enrolled. Early studies often focus on the easiest patients to measure, not the hardest to treat. That can make a therapy look cleaner than it will in everyday care.
For patients, the practical move is still the same. Ask about your current LDL goal, whether your risk level justifies more aggressive treatment, and whether newer options fit your case. The future may be arriving, but your heart risk is being managed now.
Where LDL gene therapy goes from here
The next few years will tell us whether this is a genuine advance or a clever detour. If the therapy keeps LDL down safely, for long periods, and at a price health systems can absorb, it could reshape cholesterol treatment. If not, it will join the long list of ideas that looked stronger in a press release than in practice.
That is the real test. And it is the one that still matters most.